|
|
 |
 |
|
|
| Successful treatment experience of acute antibody mediated rejection using bortezomib: A case report |
|
|
|
| Department of Pathology, Yeungnam University College of Medicine, Daegu, Korea |
|
|
| Department of Internal Medicine, Bong Seng Hospital, Busan |
|
|
|
|
|
Antibody-mediated rejection (AMR) has recently been recognized as an important cause of early renal allograft dysfunction because it is frequently unresponsive to conventional antirejection treatment. We herein describe our experience with the use of bortezomib as a rescue treatment who developed AMR that was refractory to a combination of rituximab, steroid, plasmapheresis and intravenous immunoglobulin.
A 42-year-old woman with graft failure started hemodialysis for five years before her second transplantation; 3/6 antigen (A, B, DR) mismatched deceased donor. For the first transplantation, she received living donor kidney from her mother 15 years ago for her diabetic renal failure.
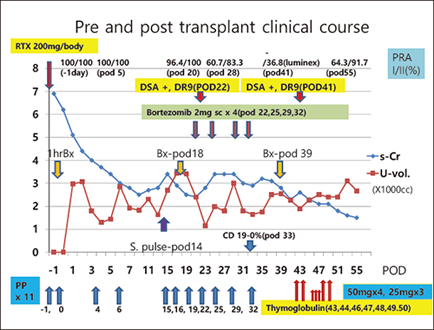
She was treated preoperatively with rituximab (200mg/body) and two times of plasmapheresis (-1 day and operation day) because her preoperative panel reactive antibody (PRA) by ELISA screening was 100% Class I and 100% Class II and previous 15 times of cross match positivity in the waiting period. The patients received induction therapy with Simulect (IL-2 blocking agent) and triple maintenance immunosuppression therapy with tacrolimus, mycophenolate mofetil, and prednisone. An intra-operative kidney biopsy was done one hour post-reperfusion which showed faint C4d deposition in the peritubular capillaries with mild ptcitis. Plasmapheresis (x9) with low dose IVIG (2mg/kg) were done. The initial postoperative course was uncomplicated except slow decrease of serum creatinine.
On post –transplant day 15th, creatinine increased to 3.4mg/dl. She underwent the 2nd kidney biopsy, which showed type III AMR pattern (Banff ’97) without C4d deposition. The DSA showed weak HLA antibodies against DR9.
On the 22nd day after transplantation, we started four doses of bortezomib (1.3mg/m2). On the 39th day, we performed the 3rd kidney biopsy, which showed type I AMR associated with borderline acute cellular rejection (ACR). On the 43rd day, we started thymoglobulin (50mg/body x 4, 25mg/body x3) administration. Twelve days after, renal function recovered to 1.5mg/dl of serum creatinine. The bortezomib treatment was well tolerated. On the last follow-up visit (6 months after transplantation), a serum creatinine had maintained at the level of 1.5mg/dl. |
|
|
|
 |
|
|
|
|
|
戻 る ページの先頭 |
|
|
|
|
|