|
|
 |
 |
|
|
| Bortezomib Treatment for Refractory Antibody-mediated Rejection superimposed with BK virus-associated Nephropathy during the progression of the recurrent C3 Glomerulonephritis |
|
|
|
| Department of Pathology, Yeungnam University Medical Center |
|
| * |
Yong-Jin Kim、Kyung Joo Kim |
|
| Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea |
|
|
Wonseok Do、Man-Hoon Han、Sun-Hee Park、Yong-Lim Kim、
Chan-Duck Kim、Jang-Hee Cho |
|
|
|
|
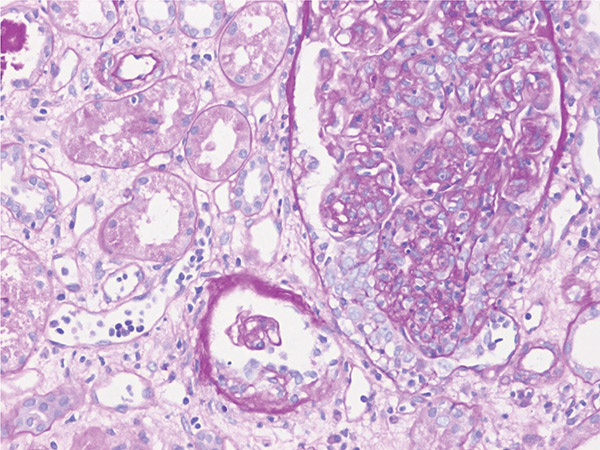
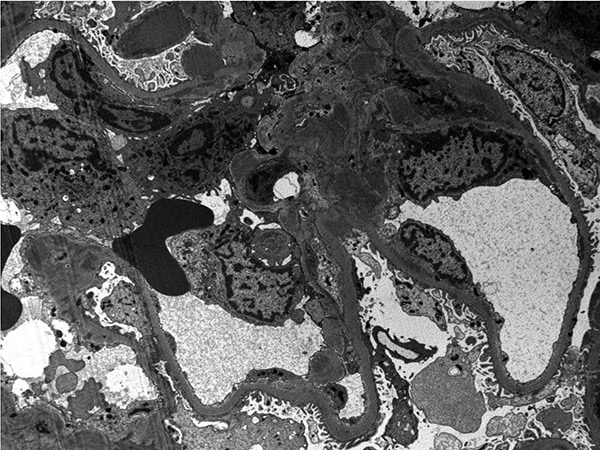
BK virus-associated nephropathy(BKVAN) superimposed with antibody-mediated rejection(AMR) is a rare but challenging condition in kidney transplatation(KT). Although bortezomib is used to treat refractrooy AMR, the impact on progression of BKVAN was not known. Here we present a case diagnosed as AMR with BKVAN during the progression of recurrent C3 glomerulonephritis(C3GN) in second KT, who showed resolution of BK viremia after bortezomib treatment.
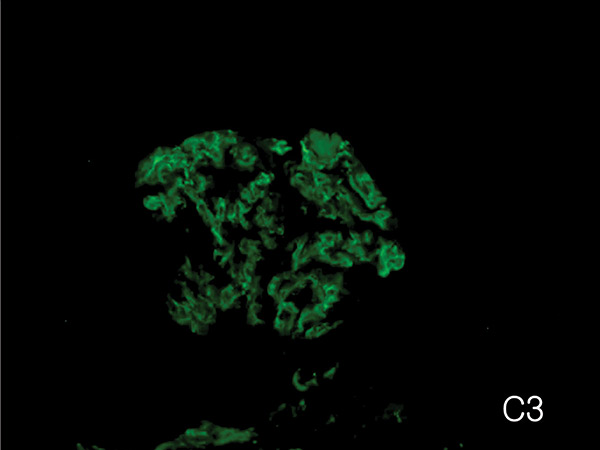
A 38-year-old man with allograft dysfunction after KT was admitted to our hospital. He was initially diagnosed with membranoproliferative glomerulonephritis(MPGN) 20 yrs ago. He received living donor KT from his father 11 years ago and was diagnosed as recurrence of primary disease one year after KT. Allograft failure developed 2 years after KT and he underwent B-cell crossmatch-positive KT(DQ7 DSA) in 10 yrs after 1st KT. During follow-up(Fig.1), the first allograft biopsy(4th month) reveald microvascular inflammation(g3, ptc1, C4d0) with recurrence of primary GN which was reclassified as C3 GN. He recieved steroid pulse, rituximab, plasmapheresis and immunoglobulin therapy. The second biopsy(10th month) showed glomerular lobular accentuation with cellular proliferation and microvascular inflammation. Same treatment was done. The third biopsy(11th month, Fig. 2, 3, 4) desmonstrated that BKVAN was complicated with the previous diagnoses. Glomerlar changes were far progressed and cellular crescents were developed. As azotemia did not improve after repeated therapy, one cycle of bortezomib (1.3 mg/m2 x 4 doses) was injected. Thereafter, allograft function stabilized and BK viremia turned to be undetectable after 6 months. The present case suggests that bortezomib therapy could be applicalbe to patients with refractory AMR even combined with BKVAN. The progression of recurrent C3 GN may contribute to this allograft dysfunction through the dysregulation of alternative pathway of complement system. |

|
|
|
|
戻 る ページの先頭 |
|
|
|
|
|





{kind=link}
{kind=link}
{kind=link}